Recognition and preemptive action against low cardiac output is one of the major challenges in cardiac surgery. Low cardiac output can be simply defined as inability of the heart to pump enough blood to meet the metabolic requirements of the body.
- Persistent acidosis = Low output
- Toes must always be warm with good pedal pulses
- A combative patient - think of low output
- Tamponade can be a cause of low output
- CI < 2.4L/m2
- Increasing Lactate > 4mmol/L
- MVO2 <65 %
- Venous pO2 < 27 mm Hg
- Increasing Toe core difference (Delta T)
- Urine output < 1ml/Kg/Hr
Prevention of low cardiac output
Cardiac output can be recognized at various stages and it is critical to prevent it and treat it in time to prevent a spiraling cycle which will be fatal It is far more important to prevent it. Prevention of low output starts from the preoperative period and extends well into the postoperative period.
Preoperative period
- Optimization of all organ systems - It is best to have all organ systems functioning optimally. Conditions like diabetes , hyothyroidism etc need to be normalized with appropriate therapy. I is well recognized that hyperglycemia , hypothyroidism are all factors that can contribute to a low output state.This may not be always possible in an emergent status but many patients can be optimized at times with a couple of hours of intensive therapy.
- Improving the energy charge of the heart - adequate nourishment of malnourished patients can improve myocardial glycogen but this may even take 10 -15 days of therapy and may not always be practical.Preoperative Glucose Insulin Pottasium infusions can be started in sick patients 24 hours prior to surgery with careful monitoruing of fluid status and Pottasium. Treatment of low cardiac output can help in decreasing preoperative low output. A preoperative IABP in patients with cardiogenic shock can help improve coronary perfusion and improve the heart prior to the CPB period. At times procrastinating and delaying surgery can actually be worse if efficient cardiac output supplementation is actually not achieved.
- Improving the energy charge of the heart - Unloading the heart with a VAD or emergent CPB can help improve myocardial perfusion.
Intraoperative Period
- The anesthesologist can reduce the myocardial work by efficient induction avoiding extremes of hypo / hypertension. The surgeon may have to establish CPB emergently / swiftly with minimal handling of the heart to reduce the period of preoperative malperfusion.
- Improving the energy charge of the heart- There may be a case for cross clamping the heart and allowing a period of aerobic arrest with metabolic supplementation(warm induction) that allows the arrested heart to improve its energy stores and prepare for a period of cardioplegic arrest. Additives that can be used like Kreb's cycle intermediates like Aspartate with Adensoine (6mg) and Esmolol(0.5 mg/Kg) can help in promoting arrest and allow the heart to repair its energy stores. It is important to give an adequate period of this perfusion and use of myocardial coronary sinus lactate (perfuse till less than 2.0 mmol/Land coronary sinus venous saturation (Perfuse till > 65 % and pO2 > 30 mm Hg) can help determine the period of warm induction
- Efficient myocardial protection- the myocardial protection strategy that worksbest for the surgeon should be used based on prior experience - this can vary from cold substrate enhanced intermitent to warm beating continuous. I (--Prasanna 18:05, 19 November 2006 (UTC))prefer to use cold maintainance (antegrade/ retrograde blood cardioplegia) with continuous (as far as practically feasible)cold normakalemic blood retrogradely with antegrade cold hyperkalemic shots at 20 - 25 minutes with normokalemic normothermic retrograde (and if possible antegrade) perfusion of the heart once critical parts of the surgery is over). This has allowed cross clamp times of 340 minutes with the ability to wean the patient off CPB with no/ minimal inotropes. Work by Buckburg and Salerno indicate that probably continuous antegrade /retrograde normokalemic perfusion on a beating heart may probably be a better option. There remains concerns by several surgeons regarding the compromise on visibility and ability to do precise repairs (especially mitral) using this techniqu. The last word on myocardial protection is anyway not out and is an evolving subject.
- Search for a mechanical correctable problem Leaving a patient with an incomplete correction leads to the possibility of low output postoperatively. Thus graft flow measurements, peroperative TEE and pressure measurements etc all can indicate an important residual problem which if left can lead to progressive low output. t is far better to spend an extra hour on CPB correcting a problem rather than face a grim situation later with worse outcomes.
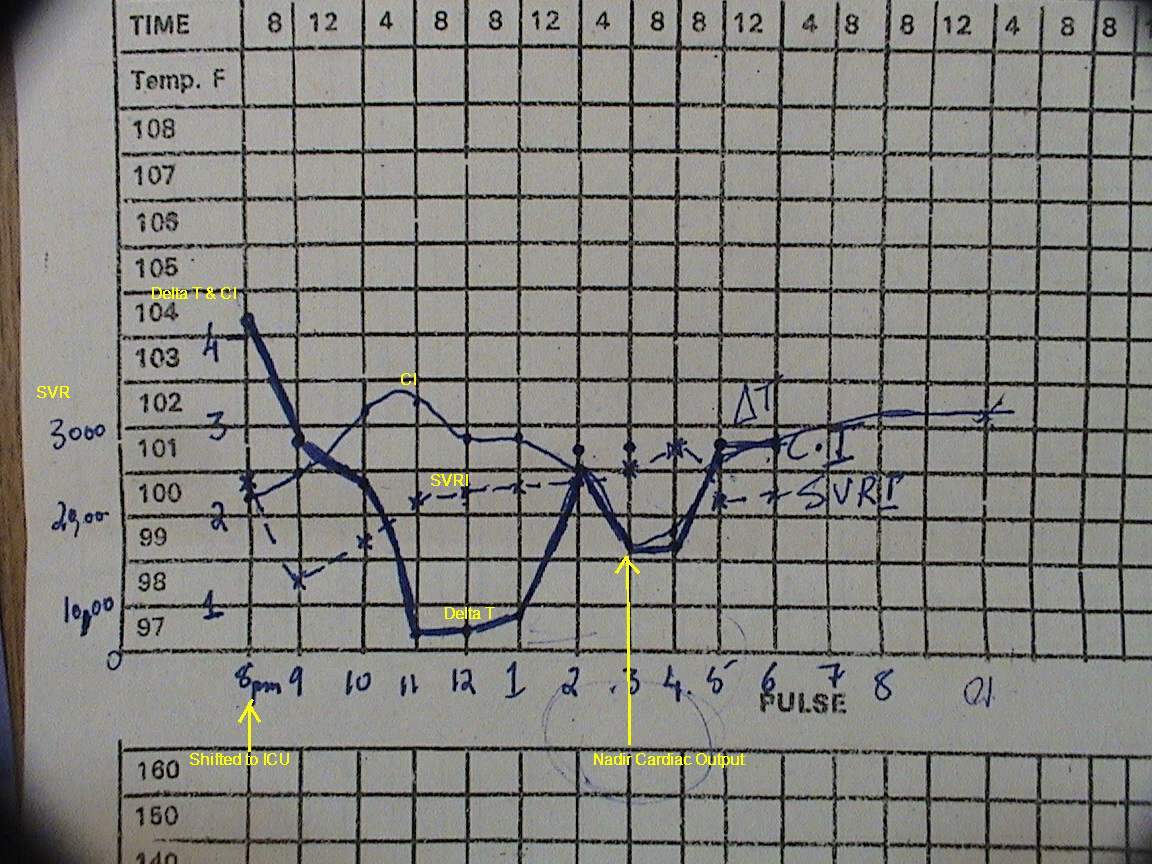
- Pre-emptive low dose inotropes and afterload reduction The point oflowest cardiac output is not at the time of weaning CPB but actually 8-12 hours later andthis dip in cardiac output can be neutralized by low dose inotrorpes and afterlaod reduction started preemptively.
- Aggressive use of mechanical assist - procrastinating in the initiation of mechanical assist in patients with cardiogenic shock can just place the patient in a vicious spiral.Some patients have obviously weak contractions but maiantain cardiac output for a a few minutes/ hours. There is no point in attempting to flog a weak horse.
- Normalisation of metabolic and hemodynamic parameters - Acid base electrolyte imbalances especially acidosis and Potassium anomalies can perpetuate low output. Beware of repeated acidosis, Hyperlactatemia with low MVO2 - and hyperkalemia - they are signs that low output has already occured
Post operative Period
{kind=link}
Post op Cardiac out put
- Early intervention for bleeding and Tamponade - It is better to re-explore earlier than late when a long period of bleeding, multiple transfusions and acidosis can make the heart inefficient.
- Correction of metabolic and hemodynamic parameters Uncorrected acidosis, high systemic vascular resistance, inadequate preload can all impair myocardial contractility.
- As discussed previously preemptive inotropes / afterload reduction and even mechanical assist (for eg IABP) can prevent the pathophysiological dip in myocardial function that typically occyrs 8-12 hours after cardiac surgery.
- Early treatment of low cardiac output can itself be therapeutic in preventing further low cardiac output !!